
The most common concern people raise before booking is whether a video call is as thorough as sitting in a consulting room. It is a fair question, and the honest answer is: there are real differences. A GP in the same room can observe things a camera cannot fully capture. What we have done is build an intake system that closes most of that gap before your appointment starts: what remains is a smaller difference than you might expect, and one that rarely changes the clinical outcome.
In this article
- Where the assessment actually happens
- What in-person has that telehealth may not
- What a typical GP appointment looks like
- What our process looks like instead
- How the intake is built to work for ADHD brains
- Why this matters more for women
- What the GP sees before you speak to them
- Frequently asked questions
Where the assessment actually happens
ADHD is not diagnosed by observing behaviour in a 45-minute appointment. It is diagnosed from a clinical picture built before you speak to the GP: questionnaire scores, personal history, observer report, and childhood evidence. That preparation happens the same way regardless of whether your appointment is online or in person.
ADHD is a chronic pattern across multiple settings over years, not a set of behaviours observable in a single consultation.
When people worry about telehealth, they imagine a GP watching them on a screen, trying to spot signs of ADHD. That is not how ADHD is assessed. ADHD is a chronic pattern across multiple settings over years, not a set of behaviours observable in a single consultation.
What in-person does add is physical presence. A GP in the room can observe how you move, make eye contact, notice things a camera angle or connection quality might not transmit. We cannot replicate that through a screen. What we can do is ensure the clinical data collected before the appointment is thorough enough that the diagnostic picture does not depend on those 45 minutes of observation. The intake is designed to surface what observation alone would miss.
What in-person has that telehealth may not
When we say telehealth, we mean two things: your intake through the Velluto app at your own pace before the appointment, and the video call itself. Together, that combination compares to in-person better than most people expect.
Physical presence in the room
- Restlessness and fidgeting visible below the camera frame
- Small motor movements, eye contact, and how someone inhabits a physical space
- The gap between how someone presents and how they feel, sometimes visible before a word is spoken
What the video call still captures: Your GP conducts a mental state examination in real time: how you speak and present, facial expressions and reactions, communication style and affect. These are established clinical assessment tools that translate to video. The medical profession recognises this, which is why Medicare funds telehealth consultations at the same rate as in-person.
Spontaneous observation before formal questions begin
- In a room, a GP observes you before the consultation formally starts: walking in, settling, how you respond
- These micro-observations can inform a clinical picture in ways that are harder to replicate on a call
What our intake does instead: By the time your call starts, the GP has already reviewed your validated questionnaire scores, personal history, and observer report. The appointment is a clinical discussion of an already-built picture, not a cold first impression. Micro-observations from a waiting room do not add much to a case built this thoroughly.
Children in a physical setting
- Children mask less than adults
- ADHD behaviours are often visible within the first minutes of a physical appointment: restlessness, difficulty settling, impulsive responses
On video, this largely holds true: Children still display signs of ADHD in video consultations. A GP who knows what to look for will notice relevant behaviour before the formal questions have begun. The camera does not significantly reduce what a trained clinician can observe in a child.
What a typical GP appointment looks like
At most practices, the entire assessment happens in the room. You arrive, explain your symptoms from scratch, and the GP forms an impression from a single cold consultation under time pressure. Most adults with ADHD have spent decades managing, masking, and compensating. In a clinical setting, many present as calm, articulate, and organised. That is precisely when the GP sees the least.
Some practices provide questionnaires at the first appointment (paper forms, or a link to an online version) and ask you to return once those are complete. That first visit costs a consult fee and gets you a form. The actual assessment then happens at the follow-up.
A paper form or a link sent by email does not change this much. You fill in what you remember, in the order it appears on the page, with no guidance on what matters or why. For someone with ADHD, a blank questionnaire under time pressure is its own problem. A better-prepared appointment is also a shorter one, and a shorter one costs you less. See how Medicare rebates apply to telehealth ADHD appointments for a full breakdown of what you can expect to pay.
What our process looks like instead
Before your appointment, you complete your intake at home with no time pressure. This covers:
- The ASRS v1.1 questionnaire (a validated rating scale measuring inattention and hyperactivity across 18 items)
- Your personal and medical history
- An observer report from someone who knows you in daily life
- Any childhood documents such as school reports
The GP reviews your complete clinical summary before the appointment starts. Your appointment (whether video call or in-person) is then a 45-minute clinical discussion of those findings, follow-up questions on specific areas, and a diagnostic conclusion.
Whether that discussion happens on a video call or across a desk is irrelevant to the clinical outcome. The GP is working from the same intake data either way. If you want to understand exactly what to prepare before your first appointment, read our guide on how to prepare for your first ADHD assessment with a GP.
How the intake is built to work for ADHD brains
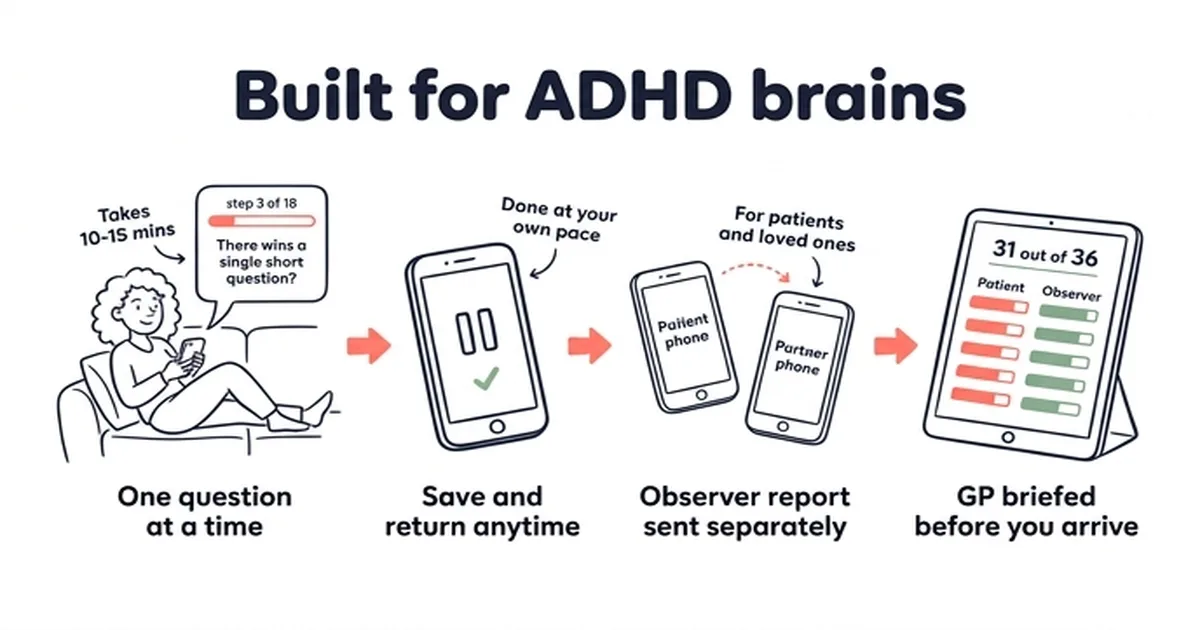
The intake is designed to be completable for someone with ADHD. Paper forms and PDF questionnaires present everything at once: a wall of questions, a blank page, a time limit. That format is its own barrier.
You access the intake on your phone and move through one question at a time. There is no scrolling past things you have not answered. No jumping ahead. Each step appears when the previous one is complete.
You can pause and return. The system saves your progress, so if you lose focus partway through, you can come back later. There is no session timeout, no starting over.
The observer report works the same way. Rather than handing a form to someone and asking them to post it back, you enter their contact details during your intake. They receive a separate link by email and complete their section in their own time, from their own device. You do not need to be in the same room. You do not need to coordinate.
Each section explains what it is for. Before the clinical questions begin, the intake tells you what that section covers, why it matters, and what kind of information is useful. You are not left guessing what “childhood history” means or whether you need to include something.
Relevant reading is linked in context. Where a section covers something patients commonly have questions about, the intake surfaces links to relevant articles. If you are not sure what observer reports involve, or what happens with your childhood documents, that information is a tap away before you fill anything in.
By the time you reach your appointment, you will have covered more clinical ground than most people cover in two or three standard consultations. Not because the questions are harder, but because the format is designed to make them answerable.
Why this matters more for women
A standard in-person appointment is the worst possible setting for women with ADHD who mask. The social pressure of a clinical environment, a doctor watching, time running out: these conditions produce exactly the kind of performance that makes ADHD invisible. Women with ADHD are more likely to mask, and masking is not deliberate. It is a learned response developed over decades of being told they seem fine.
Women with ADHD often present as calm, articulate, and composed in professional and clinical settings while managing significant difficulties in every other area of their life.
Women with ADHD often present as calm, articulate, and composed in professional and clinical settings while managing significant difficulties in every other area of their life. An in-person appointment is the setting where that presentation is hardest to set aside.
The intake done at home removes those conditions. You fill it out at your own pace, in your own space, when you choose. The questions are structured to capture the chronic pattern: the things that do not show up in a 20-minute consultation but show up every day. The observer report adds an external account from someone who sees you in real life, not a clinical setting.
By the time the GP reads your intake summary, they have a picture of how you function. Not how you present under pressure. Read more about why so many Queensland women are finally getting answers via telehealth.
What the GP sees before you speak to them
Before your appointment, the GP has already reviewed four things that a GP in a standard in-person appointment would not have.
- ASRS v1.1 scores: a validated ADHD rating scale measuring inattention and hyperactivity across 18 items
- Personal history: your current difficulties, work and relationship impacts, medical history, and medication review
- Observer report: an account from someone who knows you well (a partner, sibling, or close friend) capturing how your symptoms affect daily life, not how you present in a clinic
- Childhood evidence: school reports, teacher letters, childhood history confirming symptom onset before age 12, a DSM-5 diagnostic requirement
A GP walking into a standard in-person appointment has none of this. Ours has all of it before the call starts. For context on how this compares to a psychiatrist-led assessment, see telehealth ADHD assessment vs psychiatrist: what is the real difference.
This content is general information only and does not constitute personal medical advice. For advice specific to your situation, talk to your GP or another qualified health professional. Information current as of April 2026.
Frequently asked questions
Can a GP diagnose ADHD via telehealth in Australia?
Yes. In Queensland since December 2025 and South Australia since February 2026, specialist GPs with FRACGP diagnose and prescribe for adult ADHD. Telehealth appointments are covered under the same Medicare framework as in-person consultations and carry the same clinical and legal weight.
Will the GP be able to tell I have ADHD from a video call?
Your GP does observe you during the video call: how you speak and present, your facial expressions and reactions, your communication style and affect. That is real clinical observation, and part of why telehealth is accepted as clinically equivalent to in-person by Medicare and the medical profession. What ADHD is not diagnosed from is observation alone in a cold consultation with no preparation. Because your intake is complete before the call starts, the GP is working from a full clinical picture, not a first impression.
Does masking affect a telehealth assessment?
Masking affects any assessment that relies on observation during a consultation. Our intake is completed at home, at your own pace, before you speak to anyone. The GP reviews a complete clinical picture before your appointment. Masking during the appointment itself does not affect the diagnostic process.
Is an online ADHD diagnosis accepted by Medicare and the PBS?
Yes. A diagnosis from a specialist GP qualifies for Medicare rebates and PBS-listed medication under the same rules as any other GP consultation.
Why does the observer report matter?
The observer report gives the GP an account of how your symptoms affect your daily life from someone who sees you regularly, not how you present in a clinical setting. For adults who mask, it often contains information that would never come up in a standard consultation.
What if I do not have childhood documents?
Childhood documents such as school reports and teacher letters are useful but not always required. The GP assesses the full clinical picture including your recall of childhood symptoms and the observer’s account. If documentation is unavailable, discuss this at your appointment.
General health information
This article is general health information only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always speak with a qualified health professional before making any changes to your medication or treatment plan.
MySpecialistGP is a health information and GP directory service operated by Webbed Feet Pty Ltd. Read our Medical Disclaimer.